Hello, everyone...
The next topic is usually infrequent, and is the clinical presentation of the pathology known as "Rabdomyosarcoma" which is described as a neoplastic entity with malignant characteristics that originates from previously healthy skeletal muscle cells.
Rhabdomyosarcoma is a typical childhood neoplasm that originates in embryonic mesenchymal cells that have the ability to differentiate into skeletal muscle cells, which is why they can develop in almost any type of muscle tissue and have a very variable location and clinical manifestations.
This neoplasm represents the three causes of soft tissue cancer in early ages with an incidence from 5 years of life to 21, obtaining its highest peak at 15 years and these being those of gloomy prognosis. It most often affects males and whites.
Although the genetic factors that predispose the appearance of this malignant pathology are not very clear, it is associated with entities such as neurofibromatosis type I, Li-Fraumeni syndrome, costello syndrome and Beckwith Wiedemann syndrome. On the other hand, environmental factors have been determined, such as exposure to ionizing radiation, chemical agents, some oncogenic viruses and the consumption of illicit substances such as cocaine and marijuana increase the risk.

Medical consultation. License: CC0 Public Domain
Histology
The muscle cell or muscle fiber represents the functional and structural unit of muscle tissue. It is a specialized type that is in charge of protein synthesis in this case actin and myosin. These can be electrically and chemically stimulated, just like nerve cells.
According to their function, form, disposition and structure, muscle cells are grouped into 3 categories:
Smooth muscle, the cells that make it up are small and have a single nucleus specialized in continuous contractions, therefore involuntary type. Most of them are located in hollow cell walls, such as the digestive tract, urinary tract, reproductive ducts, among others.
Skeletal muscle, made up of long, cylindrical cells with round and peripheral nuclei. This tissue has a striated aspect and are responsible for the movements of the skeletal system of voluntary type.
Cardiac muscle, with the following characteristics; acidophilous, short, cylindrical and branched, with one or two nuclei, with the appearance of striated muscle. It is of involuntary type, they are typical of cardiac tissue (heart).

{kind=link}
Histology muscle cells. Author CNX OpenStax. Attribution 4.0 International (CC BY 4.0)
Anatomy
Pelvis
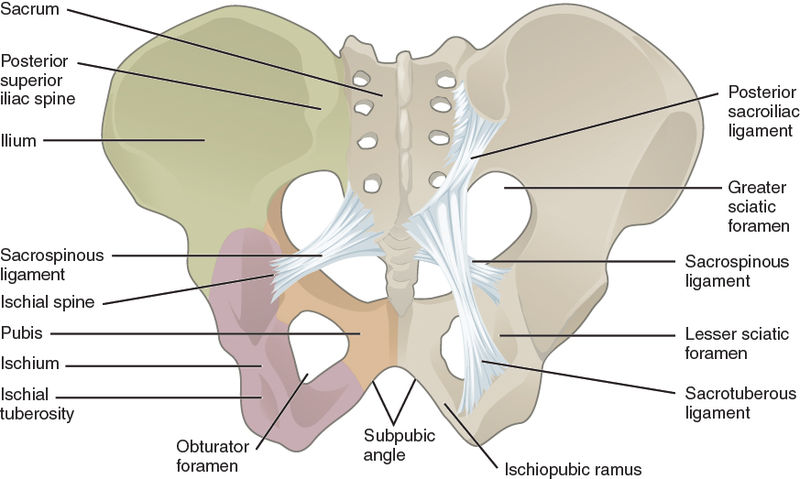
This important portion of the human body is represented by four bones, the sacrum, the coccyx and the two iliacs.
There is an imaginary line also called the terminal or unnamed line that limits the false pelvis of the true one. The false pelvis is delimited at the back by the lumbar spine and at the sides by the iliac fossa and at the front by the lower portion of the abdominal wall. While the true pelvis is below the terminal line delimited above with the promontory, the wings of the sacrum and pubis, below with the inferior narrow of the pelvis.
The pelvic waist is made up of the ilium, ischium and pubis, it provides protective functions and contains viscera such as the bladder and genital organs, as well as promotes posture and movement.
Fixed and configuring stability to the pelvis ligaments, sacroiliac dorsal and anterior ligament, supraspinatus ligament and tuberous sacral ligament. In relation to the muscles present in this portion of the human body are pyramidal (pyriform) internal obturator.
{kind=link}
Pelvis anatomy. Author OpenStax College. Attribution 3.0 Unported (CC BY 3.0)
Rhabdomyosarcoma
As already described there are 3 types of muscle cells, in the present article we will take into account the main groups, smooth muscle cells of involuntary type and striated muscle cells or voluntary musculo-skeletal type. "Rhabdomyosarcoma" originates from healthy muscle cells, which is why it can be located in any area of the body that has this type of tissue.
This malignant neoplasm can develop in almost any potion of the organism, but has a predilection for certain parts:
- Head and neck (35%) taking into account the orbit and nasopharynx.
- Urogenital system (25%) bladder, prostate and vagina.
- Both upper and lower extremities (20%).
- Trunk and others (20%).
- Injuries to the face and neck that compromise the orbit of the eye and nasopharyngeal usually lead to eye pain, tearing, nasal congestion, dysphonia and seropurulent discharge.
- Urogenital injury, abdominal pain, compressive symptomatology (paresthesia, loss of muscle strength among others) palpable mass, difficult for urination, among others.
- Injury in extremities are characterized by palpable lesions, poorly defined stone painless and adhered, often generate metastases to nearby nodes, bone, bone marrow and lung.
- Laboratory examinations where leukositosis is observed with blnacas beads 15.000 at the expense of Seg 80% with haemoglobin of 10 and platelets: 350.000 within normal limits.
- Renal and hepatic functionalism without alterations. In relation has positive acute phase reactants with a VSG 65 and elevated indirect markers LDH 977 alkaline phosphatase 202 Calcium 9.7.
- Pelvic LOE for left medial: SARCOMA?.
- left hydronephrosis.
- of the study without pathological findings.
- Muscular planes, aponeurosis without alterations.
- Blood vessels of normal trajectory and caliber.
- Inguinal canal without alterations.
- Hyper-echoic oval image of approximately 3cm x 2.1cm is evident in relation to adenopathy.
- Genetic Modeling of Human Rhabdomyosarcoma. Corinne M. Linardic, Diane L. Downie, Stephen Qualman, Rex C. Bentley and Christopher M. Counterlink
- What is rhabdomyosarcoma?. Author: Amelia F Drake, MD; Chief Editor: Arlen D Meyers, MD.link
- Oral rhabdomyosarcoma: A review Ankita Tandon, corresponding author: Kanika Sethi, and Anand Pratap Singh. J Clin Exp Dent. 2012 Dec; 4(5): e302–e308.link
- Childhood Rhabdomyosarcoma. Recent Advances and Prospective Views C. Wangcorresponding author. J Dent Res. 2012 Apr; 91(4): 341–350.link
- Rhabdomyosarcoma in adolescent and young adult patients: current perspectives. Daniela Egas-Bejar and Winston W Huh. Adolesc Health Med Ther. 2014; 5: 115–125.link
- Soft Tissue Tumors Brad W. Neville DDS, ... Angela C. Chi DMD, in Color Atlas of Oral and Maxillofacial Diseases, 2019link
- Rhabdomyosarcoma: An Overview Ramzi Dagher and Lee Helmanlink
- Genetics of Beckwith-Wiedemann syndrome-associated tumors: Common genetic pathwayslink
- Anatomy, Abdomen and Pelvis, Pelvis. Shazia R. Chaudhry; Khalid Chaudhry.link
- Anatomy, Abdomen and Pelvis, Sacroiliac Joint Michael Wong; John Kiel.link
- Rhabdomyosarcomalink
- Muscle Tissue and Motionlink
- Types of Muscle Tissue and Fiberslink
- Muscle Tissue and Motionlink
- Skeletal musclelink
- Smooth Musclelink
- The Muscular Systemlink
- Pelvic cavitylink
- Pelvislink
- The Pelvic Girdle and Pelvislink
Once the frequency of these primary lesions has been established by affected area, this primary neoplastic lesion is also capable of metastasizing to another system such as the lung, brain, bone marrow, ganglion, and bone.
Histopathological subtype
There are two where:
Frequent alveolar subtype with high rate of metastasis, associated with translocation t(2; 13), which fuses the PAX3 gene with the FOXO1 gene (FKHR) and t (1; 13), which fuses the PAX7 gene with the FOXO1 gene (FKHR).
Embryonic subtype characterized by loss of heterozygosis on chromosome 11p15.5.
Clinical Manifestations
Basically, this type of neoplasm does not cause fever, weight loss and night sweats (symptoms B). In general, the child or adolescent is asymptomatic or has a non-painful palpable mass, of firm or stony consistency, which can generate symptoms by compression according to its location.
The signs and symptoms are very nonspecific because, being a neoplasm of the muscle cells, then where it is generated the symptomatology.
Diagnostic
Emphasis has always been placed on a good medical history, and physical examination, which guides us in a possible diagnosis or diagnoses.
Complementary studies of great utility are the magnetic resonance and computerized axial tomography based on the area where the lesion is suspected to be located.
The biopsy of the lesion and the immunohistochemistry allows us to establish a definitive diagnostic.

Magnetic resonance equipment. Pixabay
Treatment
It is multidisciplinary on the basis of extraction of the lesion by means of surgery as long as it is viable, in conjunction with chemotherapy and radiotherapy. Early diagnosis favors a good response and survival of life to these patients, avoiding as soon as possible underlying metastatic disease.
In general, the chemotherapy schemes used will be according to how severe the disease is, classifying it as mild, intermediate and high risk. Using in most cases cycles with vincristine, cyclosphophamide, actinomycin, or certain cases with doxorubicin ifosfamide and etoposide.
Clinical case
This is a 15-year-old female patient, with no known pathological history, who reported onset of current disease in mid-September 2017, characterized by presenting moderate pain intensity, located at the level of the left hip joint, without irradiation, with constant pain, and does not give way with common analgesics, with progressive clinic of 3 weeks of evolution, which is associated with arthralgia of mild intensity in right hip joint, which in turn radiates to right ankle and left knee, with slight increase in these joints without sign of phlogosis, which is accompanied by functional limitation and gait impairment, treats with common analgesics without satisfactory response.
At the beginning of January 2018, there was an increase in volume in the internal portion of the left gluteus, without signs of phlogosis and very painful, which is why it was taken to a private physician who indicated treatment with pregabalin 75mg, prednisone 5mg VO OD and meloxican 15mg VO, being treated under the context of juvenile Idiopathic Arthritis, in view of exacerbation of the clinical picture with subsequent complete limitation of walking, decided to abandon treatment one day prior to admission.
At the beginning of February, in the afternoon he presents generalized tonic clonic movements, concomitant ocular retroversion, relaxation of the vesical sphincter and loss of consciousness of approximately 10 minutes, reason for which he is brought and after evaluation he is admitted to complete studies.
The patient has no personal or family history of great importance, in turn do not consume tobacco or alcoholic beverages. On the other hand there is no weight loss, fever and sweating during the nights.
In the physical examination shows vital signs is observed a blood pressure of 130/80 mmHg and heart rate of 97 beats per minute, respiratory rate of 19 per minute and body temperature of 36.5 ºC.
Other important information about the patient:
Regular clinical conditions, hydrated, eupnetia, facie algide, mucosal skin paleness, tolerating oral route, ambient oxygen and decubitus, symmetrical norm expandable thorax, apex in 5th intercostal space, RsRs not ausculto murmur, audible respiratory noises in both hemitorax non ausculto added. Abdomen soft, flat, painless RsHsAs present, no visceromegaly.
In left inguinal region mobile adenopathy is palpated, painful to the mobilization of smooth surface of approximately 2cm, not adhered to deep planes. Normoconfigured genitalia on the internal face of the left gluteus, which takes the perineum and vulva, a significant increase is evident, with no sign of phlogosis, a stony consistency, a regular surface and no pain on palpation.
Extremities without edema, mobile. Conscious neurological, oriented in time, space and person, without alteration of cranial pairs, muscular strength preserved in upper limbs, lower left limb III/V and lower right limb IV/V alteration of epicritic touch in an asymmetrical way and alternating to right predominance, without meningeal signs.
In view of the patient's signs and symptoms, the following complementary studies are requested:
SEROLOGY FOR HIV BY ELISA METHOD (NEGATIVE).
Abdominal and Pelvic Echogram:
Ultrasound of skin and soft tissues in left inguinal region:
Biopsy of inguinal region and immunohistochemia ganglia: reports embryonic rabdiomisarcoma.
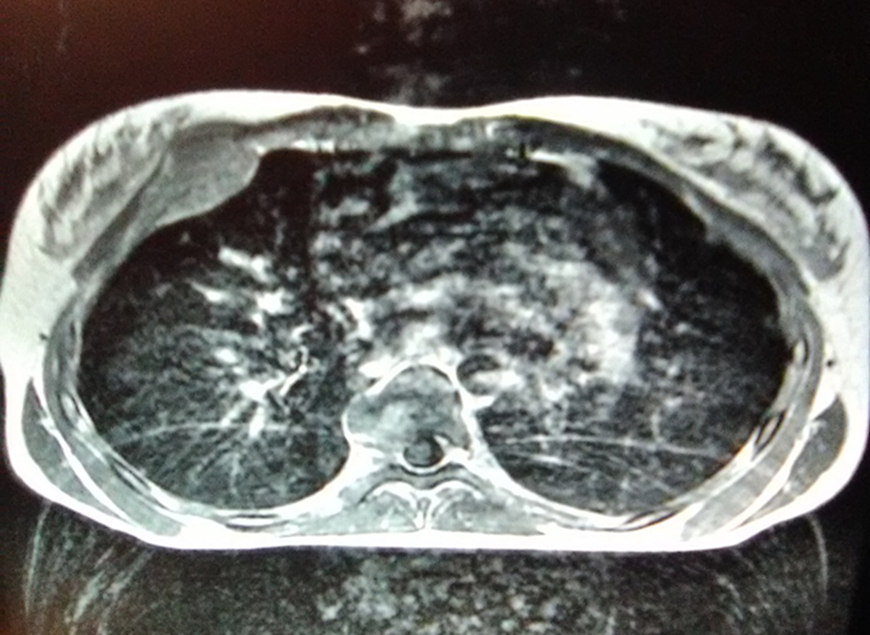
ONCOLOGIC TRACKING WITH MAGNETIC RESONANCE IN THORAX, ABDOMEN AND PELVIS.
Magnetic resonance of thorax:
@anaestrada12
Conclusion: at mid mediastinal level in pulmonary aorto window, retrocave and subcarinal multiple hypo-intensity nodular images measuring 3.3 cm, 2.8 cm and 1.8 cm respectively in relation to lymph nodes.
@anaestrada12
Conclusion: at the level of the anterior thorax that impresses the costal arch, an oval-shaped space-occupying lesion is observed, with defined edges that condition anterior displacement towards soft tissues. Fracture of vertebral body T5 is observed.
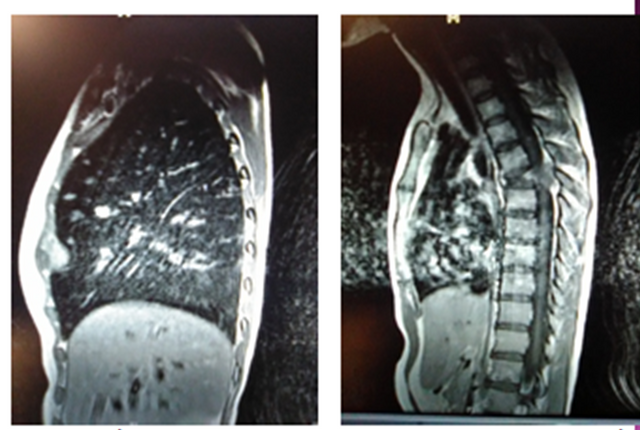
Abdominal Magnetic Resonance

@anaestrada12
Conclusion: no alterations or evidence of pathological lesions. At left kidney level slight pyelocalicial dilatation (hydronephrosis grade I). Displacement and fracture of vertebral bodies L5-L4 is observed.
Pelvic Magnetic Resonance

@anaestrada12
Conclusion: at the level of the pelvic fossa there is a space-occupying, lobed lesion with regular, well-delimited edges. Isointense in T1 and heterogeneous in T2 FATSAT to hyperintense predominance with hydric restriction in diffusion, conditioning cephalic and anterior displacement of uterus and ovaries.
Final conclusions
To get into the subject, you must take into account that rhabdiomisarcoma belongs to the groups of tumors called soft tissue sarcoma, and that these are malignant tumors originated from mesenchymal cells, which when they reach the necessary maturity are differentiated and become what is known as skeletal muscle, smooth muscle, adipose tissue, connective tissue, bone and cartilage.
However, Rhabdomyosarcoma is a malignant tumor that originates from skeletal muscle cells, both smooth and striated muscle, which allows it not to have a specific location, however, it is described that more often are located in the head and neck structures (almost 40% of total cases), the male or female genitourinary tract (about 25% of the total) and extremities (accounting for about 20% of cases).
The clinical presentation of Rhabdomyosarcomawill depend on its location, for example, if it is located in structures of the head such as the orbit, it is usually accompanied by a protruding or swollen eye (proptosis), usually accompanied by this infection (pain, fever, purpuric coloration of the eye). In our case the location is pelvic and therefore the clinic presented by our patient.
Histologically, Rhabdomyosarcomais divided into several subtypes: embryonic, alveolar, and other cell subtypes pleomorphic or anaplastic, mixed and fusiform cells. Therefore, the diagnosis of this entity is based on biopsy of the lesion.
In relation to the prognosis, it is usually better for patients from 0 to 4 years old, with small tumors (less than 5 cm) while, in older patients, larger lesions, and metastatic, as in the case presented, the prognosis is reserved. And they deserve to start chemotherapy and radiotherapy, manage pain and quality of life.
Sources:

steemSTEM is a project of the chain of blocks that supports the scientific content in different areas of science. If you want to know more about this wonderful project you can join the server in discord
This article will be published at https://www.steemstem.io/
link
I hope you enjoyed my content.
Originally posted here: https://steemit.com/steemstem/@anaestrada12/diagnostic-of-pelvic-1572312084
No comments:
Post a Comment