Attention: Some people may be sensitive to the images presented in this article.
Greetings beloved steem platform, as usual every week, today I would like to share a very common topic, as a reason for consultation in emergency rooms and outpatient consultations. These being one of the skin and soft tissue infections called Erysipela Ampollar, whose characteristics, symptoms and treatment will be discussed below.
We must start talking a little about the skin, which as we all know is the largest organ of the human body, with an essential function that is the protection of the body against various external agents, call bacteria fungi, parasites and even sudden changes in temperatures and certain substances.
The Erysipela`s, is an infectious disease of bacterial origin, which takes the epidermis, dermis and in some cases severe the hypodermis, the germs mostly involved are gram positive, as is the case of streptococcus. With acute presentation and touch of the general state if the infection is allowed to progress, which in the beginning is only local.
Generally, it affects both men and women without predilection for any, with respect to the affected age group, it is usually more frequent in the extremes of life, ie pediatric ages and older adults over 55 years.
To talk about infectious processes we must know the characteristics and composition of the skin which we will develop next.
Composition of the skin
As already mentioned, the skin is the largest and heaviest organs, which covers the human body, with essential functions ranging from protection against external agents such as heat, cold and microorganisms, as well as being responsible for the balance of body fluids.
The skin is rich in vascular and sensitive innervation, which is why we can express our emotional state as, for example, when we blush, pale skin, and pheromone secretion.
The skin is made up of several layers:
- Firstly, it is located, the epidermis is the layer that first comes into contact with the environment, constituted by a stratified and keratinized poly squamous epithelium, allowing it to have strength and resistance.
- Dermis is the next layer, formed by fibroelastic connective tissue which allows it to provide support, resistance and elasticity, in addition to nourishing the epidermis and has a rich vascularization.
- Appendices of the skin, represented by; hair, sebaceous glands, sweat and finally nails.
- Subcutaneous tissue or hypodermis with variable thickness and which is constituted by numerous nerve endings and blood vessels. It represents a source of energy storage, thermal insulation and mechanical protection.
-
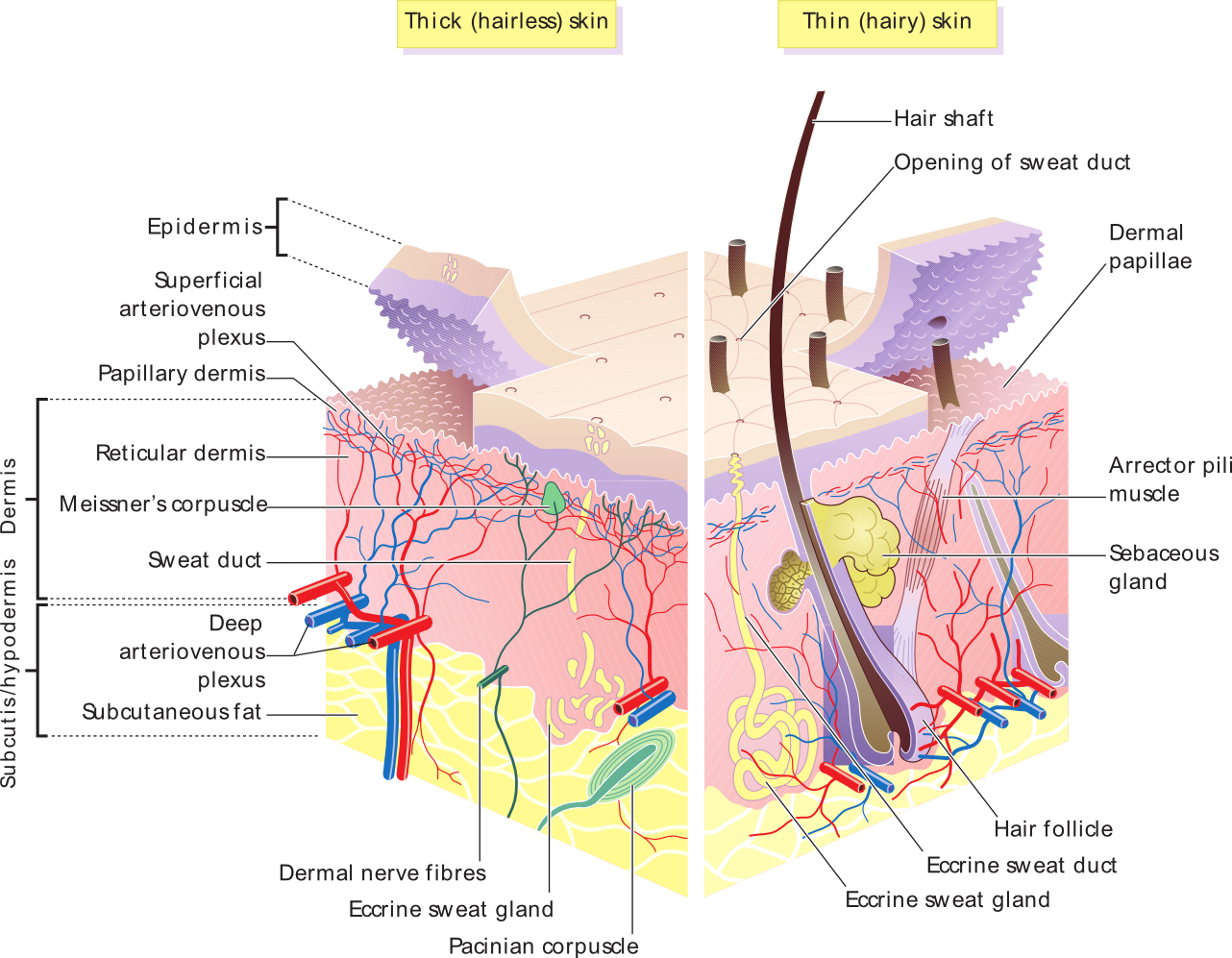
Skin layers. Public domain image author: Madhero88. Licensed CC0 1.0
Erysipela Ampollar
This infectious disease of bacterial cause, being the germs involved the Gram positive, with acute clinical and presentation of local lesion after 48 hours or less. In the early stages, it only represents a local infection, which, if not treated, becomes systemic with a commitment to life.
It affects the lower limbs more frequently in more than 95% of cases. In early stages we can observe edema, flushing and heat in the affected area with subsequent presence of blister-like lesions and presence of serous secretion.
If it is treated early, at an early stage, the symptoms are usually only local and even without the presence of fever, but if it is not treated, the infection progresses to become systemic, and there is a compromise of the general state.
Etiological agent
The skin has its own bacterial flora, which protects it from the external environment, but nevertheless, in certain opportunities, this own flora is capable of producing infection.
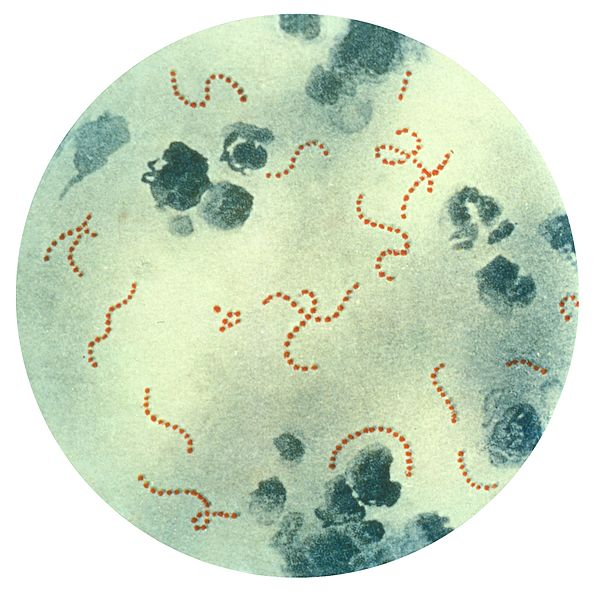
Streptococcus pyogenes and Staphylococcus aureus are usually the most involved germs, which under certain circumstances, such as open lesions on the skin, allow entry to deeper layers and cause infection. However, for this to happen there must be an immunological deficit.
Most literatures associate them in groups such as:
- Group A beta hemolytic streptococcus, and groups B, C, D and G.
- Staphylococcus aureus (isolated more frequently in diabetic patients and facial localization) less frequently.
- Pseudomonas aeruginosa and enterobacter, associated with nosocomial infections.
-
Pathophysiology
Basically this bacterial infection is caused by streptococcus in the first instance. Generally this type of pathology is associated to Streptococcus pyogenes, Streptococcus agalactiae and less frequently Staphylococcus aureus.
Our skin to be broken by an injury that generates loss of the continuity of the same and therefore disruption of the cutaneous barrier allows that bacteria already mentioned that is part of the bacterial flora of the skin in its outer layer, penetrate and cause local infectious processes.
Streptococci have properties that attribute their capacity for virulence, as is the case with the M protein and the capsule, which allows it to delay phagocytosis, facilitating its penetration into adjacent tissues.
They also have the capacity to originate exotoxins and enzymes which are responsible for triggering local inflammatory processes. The exotoxins elaborated in the erysipelas are SpeB and SpeC, responsible, as already mentioned, for inflammation and local cell death.
Predisposing factors
All that skin lesion capable of originating an entrance door, by means of the disruption of the cutaneous barrier, for example:
- Surface wounds such as tearing or scratching.
- Skin ulcers.
- Wounds opened by sharp objects or trauma.
- Mycotic lesions.
- Presence of varicose veins and lymphedema.
- Alcoholism, diabetes mellitus and obesity.
- Diseases that generate immunological alterations, systemic lupus erythematosus, rheumatoid arthritis, among others.
- Extremes of life for older adults and pediatric ages.
-
Clinical manifestations
Sharp presentation and rapid evolution, if not treated in time.
It begins with a local infection caused by flushing, heat and edema, followed by an erythematous plaque which progressively extends and finally the presence of blisters and blisters with abundant serous secretion.
It is usually unilateral, with predominance of lower limbs.
It may be accompanied by systemic symptoms or not such as; fever, headache, hyporexia, asthenia and chills.
Diagnostic
Exclusively clinical, physical examination and medical examination.
Laboratory.
It can present with leukocytosis at the expense of neutrophilia. VSG and PCR positive.
Determine renal and hepatic function.
Metabolic controls in the case of having a history of diabetes mellitus, or ruling out the presence of it.
Cultures of secretion of phlyctenules and blood cultures should be requested if necessary, in severe cases of septicemia.
Treatment
Simple will depend on the physical state and extent of the injury.
Those tables of early local infection only if it touches the general state, can be considered outpatient treatment with oral treatment, based on DICLOXACILINA, CEFALEXINA, CLINDAMYCIN, AMOXICILLIN-CLAVULÁNICO, OXACILINA.
Moderate to severe cases or patients with decompensated-based comorbidities that require parenteral treatment; CRYSTALLINE PENICILLIN continues to be the gold standard in this pathology, as alternatives, 3 and 4 generation cephalosporins, fluoroquinolones, clindamycin, and macrolides.
In cases where it is suspected that the isolate is methyl resistant, treatment with Vancomycin is ideal.
Real clinical case report
A 69-year-old male patient with a history of type 2 diabetes mellitus and arterial hypertension, who reported about 5 days ago an increase in the volume of the lower right limb, accompanied by blushing, heat and functional limitation, likewise two days later associated with type lesions. flictena and blister to predominance of internal face of the extremity, concomitant fever to 39º C, that yields with common antipyretics, polidipsia, polifagia and nocturia so it is valued and entered.
The positive to the physical examination was the presence of blister lesion in right lower limb of varying size, greater than 5 cm, with abundant non-fetid serous secretion accompanied by flushing, heat and hard edema that compromises 3 segments of said extremity.
Laboratory tests report leukocytosis at the expense of neutrophilia, elevated ESR, and metabolically decompensated hyperglycemia.
Injuries observed on the day of admission. Already described in the physical examination.



Conclusions of the case
The patient is admitted to the unit, parenteral treatment with crystalline penicillin is indicated, Gram culture is taken and antibiogram of the lesion, (awaiting results) is compensated metabolically when improving the infectious focus and initiate therapy with NPH insulin based on the calculation of His weight.
We should always recommend good skin care and cleaning, especially those patients with comorbidities that predispose the presence of infectious processes such as diabetes, encourage them to comply with their hypoglycemic treatment to lead a healthy life and that any Infectious focus go to your treating doctor in order to avoid complications.
This article is a translation of my version published in Spanish. You can read it by entering the following link: - Infección de piel y partes blandas. "Erisipela Ampollar"
-
Sources of support in the publication
- Erysipelas Wikipedia
- Erysipelas
- Functions of the Skin
- Everything you need to know about erysipelas
- How Your Skin Works
- Human skin Wikipedia
- Skin Problems and Treatments. Human Anatomy By Matthew Hoffman, MD
- Layers of the Skin
- Structure and function of the epidermis related to barrier properties
- Structure and Function of Skin
- Bacterial skin and soft tissue infections in adults: A review of their epidemiology, pathogenesis, diagnosis, treatment and site of care. Can J Infect Dis Med Microbiol. 2008 Mar; 19(2): 173–184. Vincent Ki, MD and Coleman Rotstein, MD FRCPC2
- Management of refractory Pseudomonas aeruginosa infection in cystic fibrosis. Infect Drug Resist. 2011; 4: 31–41. Published online 2011 Jan 25. doi: 10.2147/IDR.S16263. Roger Sordé, Albert Pahissa and Jordi Rello
- Synergistic Interactions of Pseudomonas aeruginosa and Staphylococcus aureus in an In Vitro Wound Model. Infect Immun. 2014 Nov; 82(11): 4718–4728. B. A. McCormick, Editor
- Streptococcus pyogenes, other Streptococci, and Enterococcus
- Streptococcus pyogenes
-

steemSTEM is a project of the chain of blocks that supports the scientific content in different areas of science. If you want to know more about this wonderful project you can join the server in discord
This article will be published at https://www.steemstem.io/
I hope you enjoyed my content.
{kind=link}
{kind=link}
Originally posted here: https://steemit.com/steemstem/@anaestrada12/-erysipela-ampollar--1558305890
No comments:
Post a Comment