This article is about the most common presentation of toxoplasma, to an organism with loss or deficit of its cellular immunity as is the case of the infection by the Human Immunodeficiency Virus.
Acquired immunodeficiency syndrome (HIV)
It is defined as the establishment of the disease caused by its etiological agent the Human Immunodeficiency Virus (HIV), which is nothing more than a positive single-stranded RNA virus with icosahedral capsule, consists of two strains (VHI-1 and VHI-2). ), which contains an enzyme called reverse transcriptase, giving it the property of integrating its DNA into the cell of the host and thus replicating itself inside.
The acquired immunodeficiency syndrome (HIV) was first described in the United States in 1981, by the Centers for Disease Control and Prevention, who in view of several unexplained cases of Pneumocystis carinii pneumonia, this being an opportunistic microorganism, in five males previously healthy homosexuals, associated with 26 cases of Kaposi's sarcoma in previously healthy men, determining that the presence of these pathological entities were secondary to an immunosuppression process, due to some type of microorganism not described.
It was not until 1983 that the human immunodeficiency virus (HIV) was isolated from a patient with lymphatic adenopathies and in 1984 it was clearly demonstrated that said virus was the causative agent of HIV
An individual could be an asymptomatic carrier or stay in HIV-priming stage for approximately 10 to 8 years without expressing the acute phase, and it is at this time that the virulence is high but the human organism has the capacity to generate a sufficient number of CD4 to counteract this process, remaining thus in a latent and asymptomatic form, only for a certain time until this balance is broken, since the time came when the immune system collapsed and the CD4 decayed, thus expressing the acute phase, which known as HIV.
Transmission Mechanism
The main route is through sexual contact in more than 80% of cases, describing other circumstances caused by cuts or punctures with instruments previously infected with blood or body fluids (semen, vaginal discharge, amniotic fluid, synovium, cerebrospinal, pleural, peritoneal , and breast milk) of patients infected with HIV. Other less frequent organ transplants and blood transfusions.
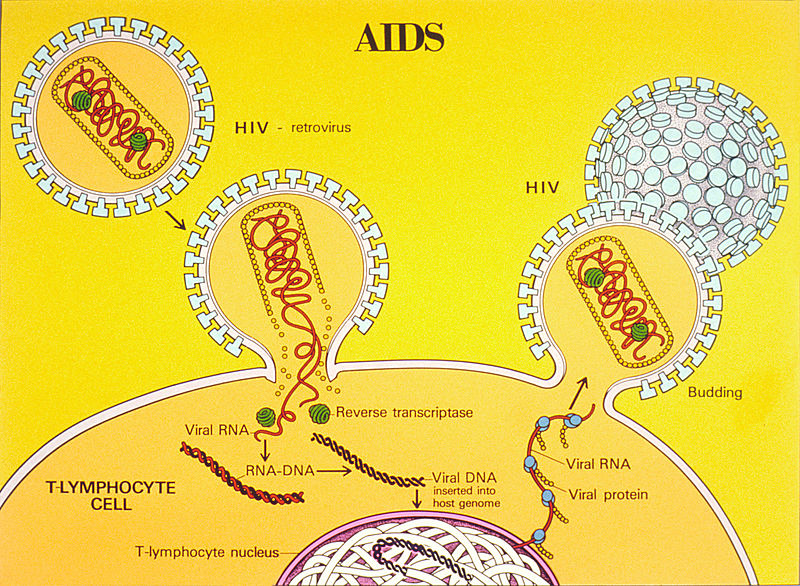
AIDS Life Cycle Illustration. Public domain image, wikipedia source CC0 1.0
Toxoplasmosis
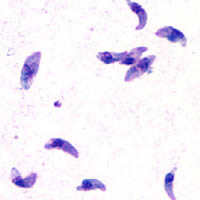
It is a disease product of infection by the intracellular parasite strict Toxoplasma gondii, is an intracellular coccidian that infects both birds and mammals, among which is man. In its life cycle there are two distinct phases: a non-feline cycle and a feline cycle.
Transmission mechanism
Through several mechanisms described below:
- Oral Transmission: the main source of Toxoplasma co-infection in humans, either by ingestion of food contaminated with feces of cats or by the ingestion of bradyzoites from pork or contaminated birds with little cooking or insufficiently frozen.
- Direct transmission (blood products / viscera): infrequent way of direct transmission of the parasite through transfusions or transplanted organs (heart, kidney).
- Transplacental transmission: only a third of pregnant women infected with T. gondii during pregnancy transmit the parasite to the fetus.
-
In general measures we must take into account that;
- When the mother is infected six months or more prior to conception, the risk is zero.
- If the infection is contracted less than six months prior to conception, the probability of transplacental infection will increase as the interval between infection and conception decreases.
- If during pregnancy the mother becomes infected in the first trimester, the transplacental infection capacity is minimal.
- If the maternal infection occurs during the third trimester, the incidence of trans-placental infection will be maximum.
-
Reproduction cycle in people
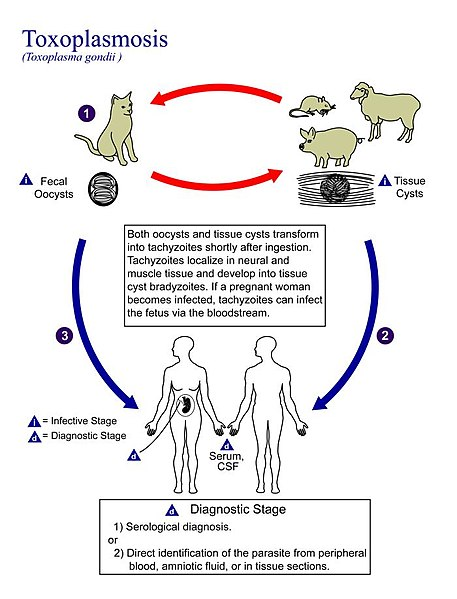
Reproduction cycle of toxoplasmosis gondii in humans. Public domain image. Author Content Providers(s): CDC/Alexander J. da Silva, PhD/Melanie Moser, wikipedia source CC0 1.0The cat is the definitive host where the stage of the sexual cycle of T. gondii takes place. Once inside the cat, the bradyzoites or oocytes expelled by the feline's feces are ingested by the intermediate host, be it HUMAN, MOUSE, SHEEP, OR PIG.
Once they enter the human organism, the cysts are quickly digested by the gastric secretions, allowing the exit of the bradyzoites or sporozoites, who have the ability to cross the epithelium of the small intestine, to become tachyzoites, which multiply rapidly and which they are capable of infecting and replicating in all the cells of mammals, except in erythrocytes.
Said parasite, when it unites with the host cell, forms the so-called parasitophorous vacuole, into which it divides. Replication of the parasite continues over and over again until the cell breaks down, releasing more parasitic forms that infect adjacent cells.
The disease in humans can take many forms, but the most important are congenital infection and encephalitis by reactivation of a latent infection in the brain of immunosuppressed individuals or the dreaded presentation as Cerebral Toxoplasmosis.
Clinical manifestations
In people with an intact immune system, acute toxoplasmosis is usually asymptomatic, goes unnoticed in 90% of cases and heals spontaneously.
Clinical manifestations by Toxoplasmosis in immunocompetent persons (integrated cellular immunity)
The most frequent manifestation is the presence of cervical adenopathy, which can be single or multiple, painless, of approximately 0.5 cm to 1 cm, they can also be located at the suboccipital, supraclavicular, inguinal and mediastinal level.
Even in some symptomatic patients it can be expressed as a lymphoproliferative syndrome ie generalized lymphadenopathy, it can be associated with headache, asthenia, fever (30ºC), myalgias, sore throat, abdominal pain, maculopapular rash, meningoencephalitis and confusion.
Among the rare complications; pneumonia, myocarditis, encephalopathy, pericarditis and polymyositis. This symptomatology can last for several weeks.
Clinical manifestations of Toxoplasmosis in immunosuppressed people
In people with a history of HIV-AIDS infection, toxoplasmosis is the main opportunistic CNS infection and its probability increases with serology for positive toxoplasmosis.
The signs and symptoms of acute toxoplasmosis of the immunosuppressed patient, with a history of HIV-AIDS infection, are expressed at the CNS level and is what is known as:
Cerebral Toxoplasmosis
The clinical presentation of this disease is secondary to the reactivation of a chronic infection and the CNS is the predilection system of this agent. It can usually be of sudden onset, or with progressive deterioration of physical and neurological status over time.
When you have a subacute clinic the patient may manifest headache (headache), fever at 39 ° C or more, malaise, and even a confusional state in days.
If the lesion is extensive enough or multiple, it can be evidenced what is called neurological focality, being the most common the hemiparesis or what equals the loss of strength of one side of the body, either right or left, as well as dysarthria, ( difficulty in articulating the word), cranial nerve involvement, which compromises visual fields, sensory alterations, which compromises gait, and even brain injury can lead to convulsive episodes.
Real clinical case
A 28-year-old male patient with a history of HIV-AIDS infection diagnosed more than 8 years ago, with no current treatment, who according to family members reported onset of illness 1 week previously, characterized by moderate to high intensity holocaranal headache, which subsides partially with common analgesics associated with a fever clinical picture at 39ºC without a predominance of hours, accompanied by hyporexia, and progressive deterioration of the neurological state expressed in drowsiness, evidenced on the day of admission with clonic tonic movements, with ocular retroversion, for approximately 15 minutes; which is taken to the emergency service.
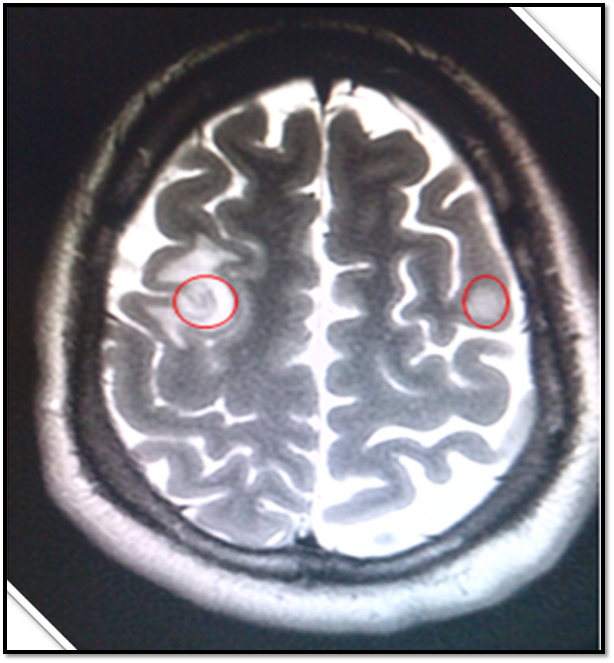
In view of the patient's clinical history and background, neuroimaging studies (Simple Cerebral Magnetic Resonance Imaging) are requested, which show the following findings.
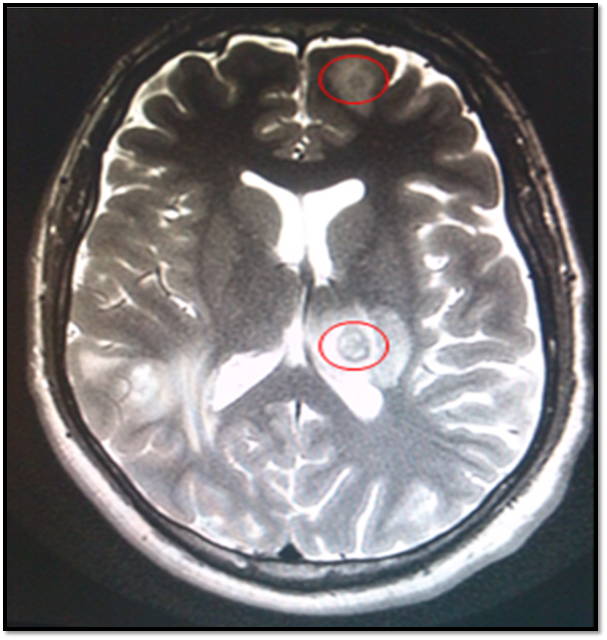

Photos property of @ anaestrada12
Conclusions of Neuro-images
It is evidenced in several cerebral Magnetic Resonance slices several lesions distributed in both cerebral hemiferios which is known as Annular Images, that is, in the form of a ring with regular delimited edges and nucleus in the center of the lesion, and marked peri-lesional edema.
Said patient, in view of the finding of resonance and history of infection with lesions similar to those described by cerebral toxoplasmosis, it was decided to start treatment with oral pyrimethamide, Endovenous Clindamycin at a dose of 900 mg every 8 hours and Leuconolver, associating the use of anti-edema measures. Dexametasone-based Brain Endovenous.
Cover image source:
- Wikipedia HIV
- Wikipedia Toxoplasmossis
- Flickr Brian
-
Sources of support in the publication
- Pathogenesis of human immunodeficiency virus infection
- History of HIV/AIDS
- A historical reflection on the discovery of human retroviruses
- Human immunodeficiency virus from the surgeons' viewpoint
- Update on acquired immune deficiency syndrome (AIDS)--United States
- Immunology of Viral Disease, How to Curb Persistent Infection
- ATLANTIC CAPE COMMUNITY COLLEGE 2017-2018. EXPOSURE CONTROL PLAN
- Appendix CRecommendations for Prevention of HIV Transmission in Health-Care Settings
- Toxoplasma gondii
- Lytic Cycle of Toxoplasma gondii
- Toxoplasma gondii: from animals to humans
- Epidemiology & Risk Factors
- TOXOPLASMOSIS
- Life Cycle - Microbiology
- Epidemiology of and Diagnostic Strategies for Toxoplasmosis
- Toxoplasmosis
- <="" a="">
- <="" a="">
- <="" a="">Lymphadenopathy
- Toxoplasmosis Testing
-

steemSTEM is a project of the chain of blocks that supports the scientific content in different areas of science. If you want to know more about this wonderful project you can join the server in discord
This article will be published at https://www.steemstem.io/
I hope you enjoyed my content.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Originally posted here: https://steemit.com/steemstem/@anaestrada12/cerebral-toxoplasmos-1559084528
No comments:
Post a Comment